Men Over 30: Understand This Before Even Thinking About TRT


Six months ago, a 42-year-old father came to me fed up. He'd been on TRT for nearly two years. His testosterone levels looked normal on paper. But he still couldn't build the "masculine physique" he wanted.
By the end of his consultation, the answer was obvious – his lifestyle was a train wreck.
Joe's story points to something the TRT industry has a strong financial incentive to obscure: most men who go on TRT don't actually need it.
After spending over a decade studying men's health, reviewing more than a dozen of the most prominent studies on testosterone decline with age, and working with men across all backgrounds to reverse low testosterone through lifestyle alone, I'm here to tell you something the TRT industry, and even your doctor, won't.
Just because testosterone declines with age doesn't mean TRT is necessary, or even beneficial. In fact, when taken unnecessarily, TRT is actively detrimental.
And even if your testosterone is genuinely low, that doesn't automatically mean TRT is the answer.
Because unless you have a genetic condition or severe testicular damage, there's really only one significant cause of low testosterone in men. And it's not aging. It's poor health.
Which means it's reversible. And yet, TRT prescriptions in the United States have quadrupled in the last decade (1).
What these men don't understand is that medicating over low testosterone without addressing the root cause first is one of the most dangerous things you can do, because low testosterone is the canary in the coalmine for almost every major chronic disease.
Coalminers used to release canaries into mines before they entered them. If the birds dropped dead, the miners knew carbon monoxide levels were too high, and it wasn't safe to enter the mine.
Taking TRT is like putting an oxygen mask on the canary – it keeps the bird alive, but it doesn't remove the carbon monoxide, which could kill the miners who follow.
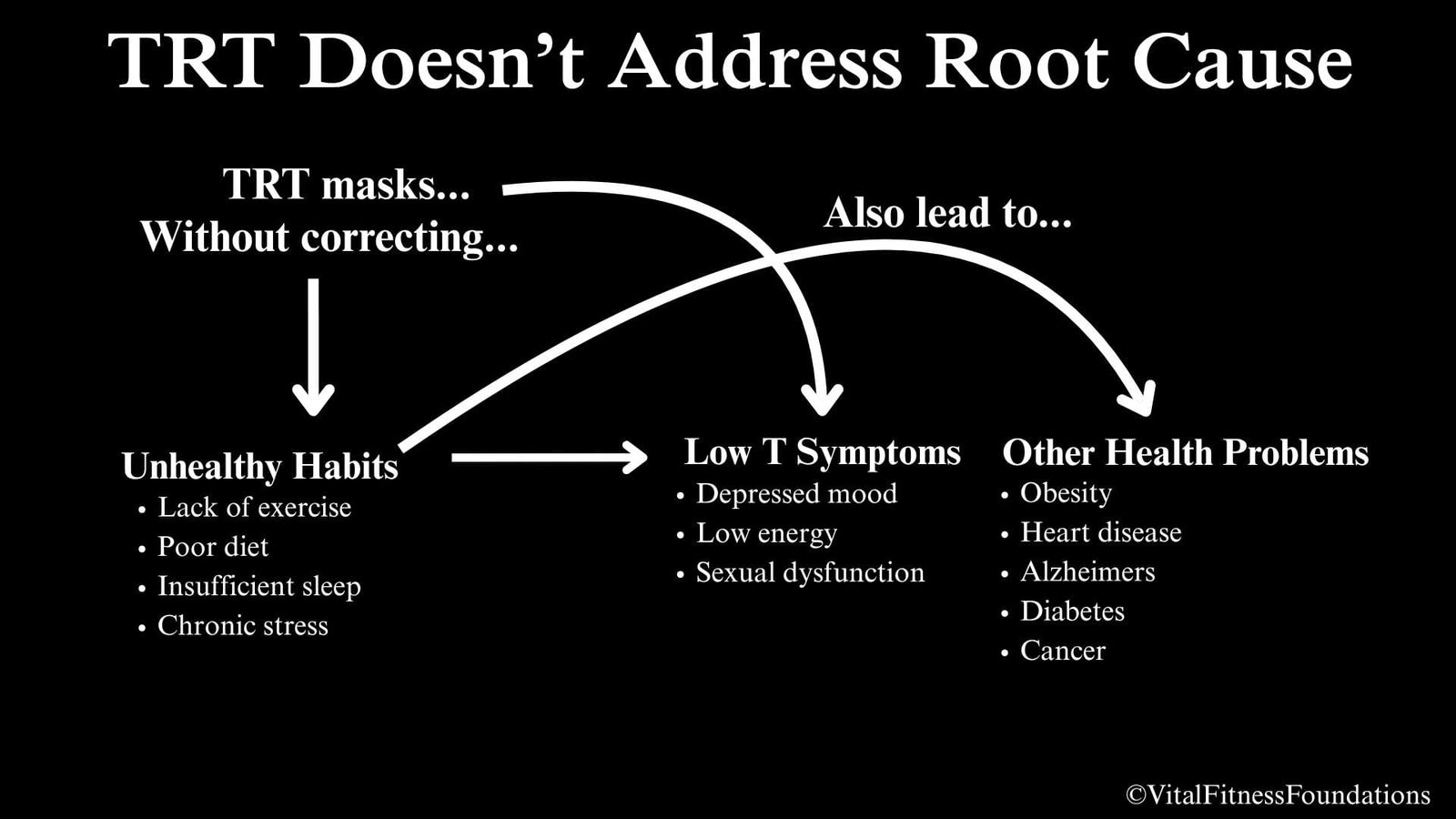
TRT can give you your libido and energy back, but it can't resolve the problems that took them from you in the first place. And those same underlying problems, left unaddressed, are the leading drivers of the chronic diseases that are quietly killing you.
That's why there's a direct connection between low testosterone and a higher risk of all-cause mortality in men (2).
Insidiously, TRT makes it less likely that you resolve the underlying problems because it removes the incentive to do so – those dreadful low testosterone symptoms. Why would you bother to address your health problems when they aren't bothering you anymore?
But there's something else TRT takes from men who don't actually need it, and it's even more costly than the health risks, because it's the defining characteristic that makes a man capable in life: his ability to confront his problems directly, solve them through discipline and persistence, and grow stronger in the process. I'll come back to Joe — because his story illustrates exactly what I mean.
In this article, I'm going to walk you through what the research actually shows about testosterone and aging, when TRT is and isn't warranted, and why most men are better served by addressing the root cause first.
Does Testosterone Really Decline With Age? What the Research Actually Shows
After writing a 7,000+ word article reviewing a dozen of the most prominent studies on testosterone decline with age, I can tell you that the narrative that testosterone declines with age has some validity, but it's often oversimplified and exaggerated.
The truth is that most testosterone decline with age is attributable to chronic diseases and comorbidities that accumulate with age, more so than aging itself.
As a result, low testosterone is more common in older men, but that doesn't mean that you're condemned to low testosterone after your 40th birthday.
It just means that your risk for developing low testosterone increases with every chronic disease that gets stacked on top of the subtle declines caused by normal aging.
Before diving into the research, it's worth clarifying what "testosterone" actually means, because not all testosterone is created equal.
Total Testosterone (TT): Represents all the testosterone in the blood, however, most (~98%) is attached to proteins called SHBG or albumin, which keep testosterone inactivated until it's released.
Sex Hormone-Binding Globulin (SHBG): A protein that tightly binds testosterone, reducing how much can be used. SHBG levels tend to rise with age, which lowers free testosterone. But it's not as simple as SHBG = bad. SHBG is a key regulator of testosterone and has important functions of its own. Albumin is a second protein that also binds testosterone but with a much weaker grip — albumin-bound testosterone can be released and used far more readily than SHBG-bound testosterone.
Free Testosterone: The ~2–3% of total testosterone that's not bound to SHBG or albumin and can immediately exert testosterone's biological effects.
Bioavailable Testosterone: Includes free and albumin-bound testosterone, representing all testosterone that is available for near-immediate use.
Dihydrotestosterone (DHT): The most potent androgen in the male body. It can be thought of as "testosterone on steroids." DHT is created when testosterone is broken down by an enzyme called 5-alpha reductase and subsequently converted into DHT.
With that established, here's what the science actually says about testosterone decline with age.
Total Testosterone
While some older studies show that total testosterone declines between 0.3% up to 1.6% starting around the mid-thirties to forties, (3)(4) multiple newer, larger studies show that total testosterone levels:
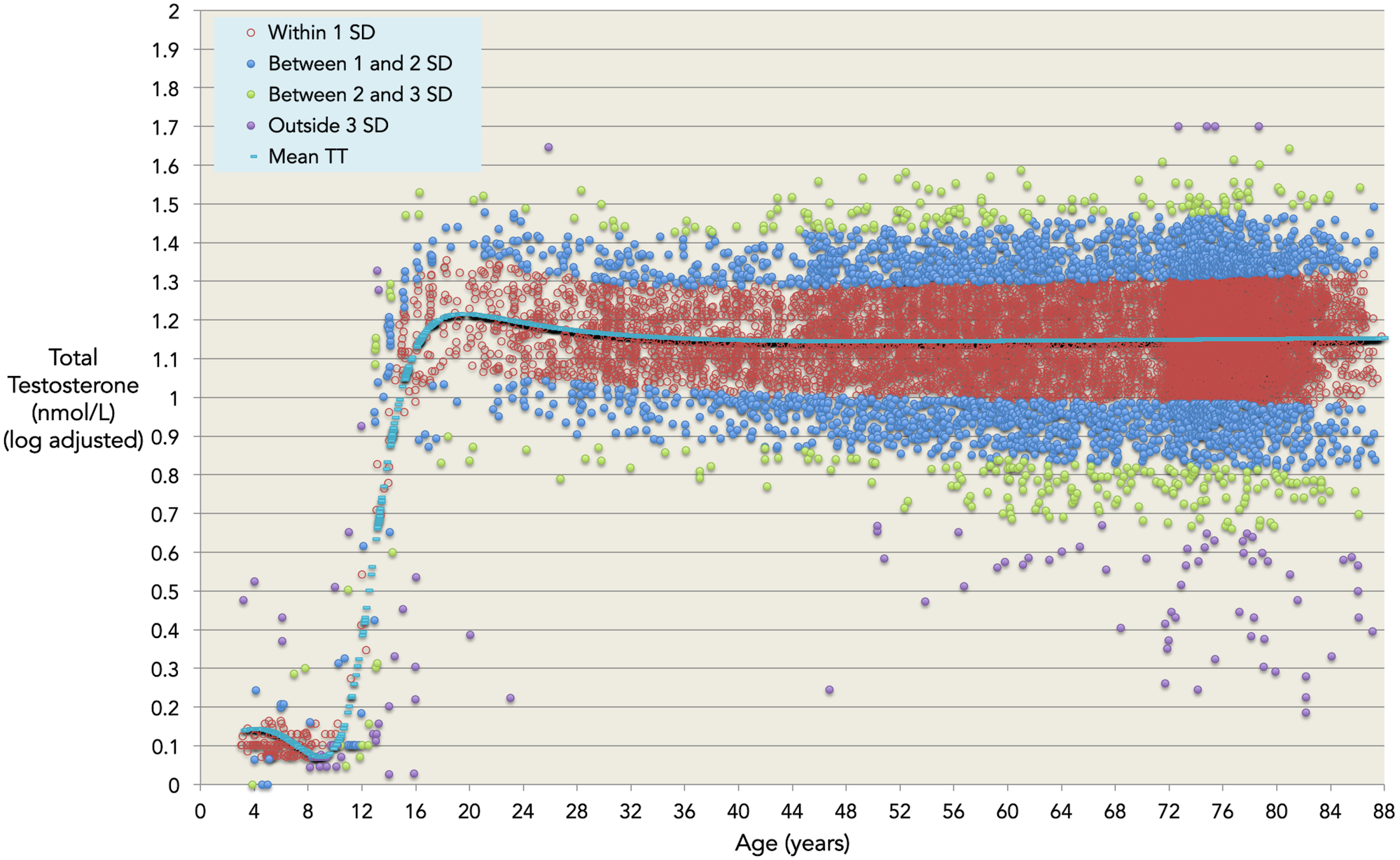
- Do not decline appreciably until after age 70–80+ (5)(6)
- Only decline slightly between early adulthood and middle age and then flatline (7)
- Do not decline at all in men 40+ (8)
Free & Bioavailable Testosterone
Free and bioavailable testosterone behave differently. In general-population cohorts they usually decline faster than total testosterone, on the order of roughly 1.3% to 3% per year, often becoming detectable by midlife, but the age at which free testosterone decline begins and the rate of those declines largely depends on a man's overall health status (9).
So much so that one Australian study on men aged 40+ who specifically self-reported being "exceptionally healthy" showed that free testosterone levels didn't decline until men reached their eighties. (8)
With the exception of that study, free testosterone does appear to decline to some degree regardless of health status, but declines do not lead to low testosterone unless exacerbated by health problems.
Dihydrotestosterone (DHT)
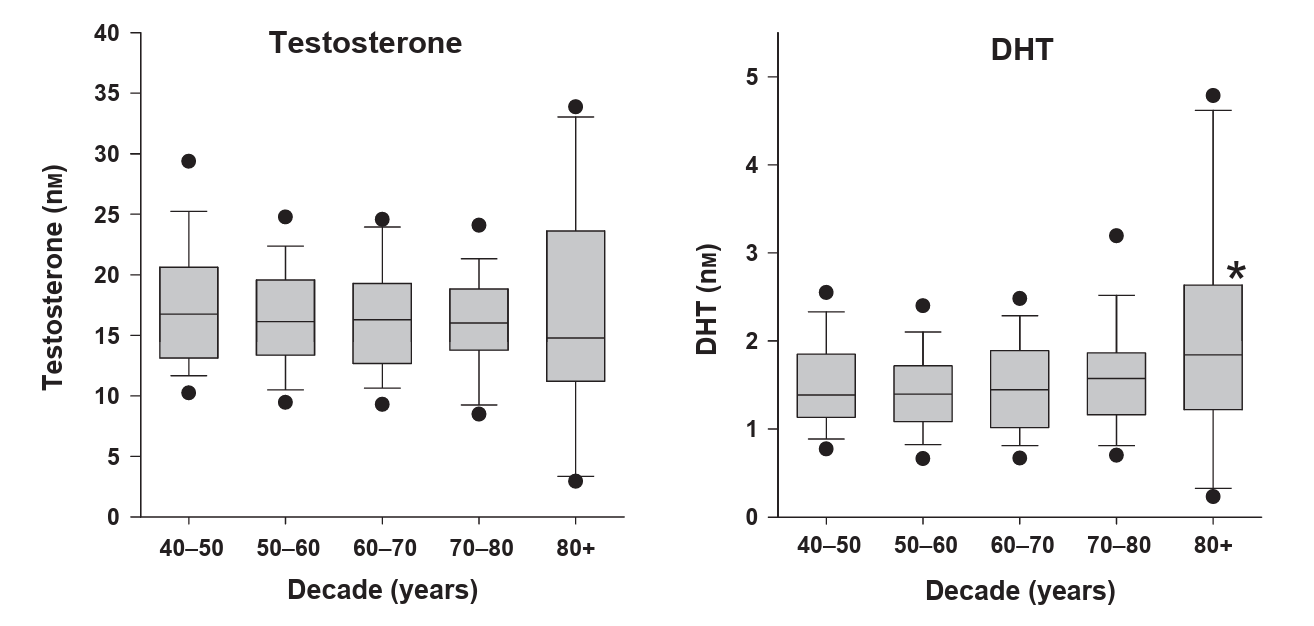
Fascinatingly, two studies reported that DHT increases slightly in healthy men (8)(3).
Since DHT is the most potent derivative of testosterone, researchers posit that this may be a compensatory mechanism the body uses to keep overall androgenic status elevated.
The most important takeaway is that your overall health is the most potent determinant of the degree to which your testosterone levels will decline with age.
Therefore, men who avoid developing chronic diseases and comorbidities can expect total testosterone to remain relatively stable throughout life, whereas free testosterone will likely start to dwindle around late-middle age, but will remain eugonadal (in the healthy range).
To the contrary, men who don't take care of themselves and accumulate health problems as they get older will experience declines in both types of testosterone earlier, and to a greater extent – drastically increasing the risk of developing late-onset hypogonadism (low testosterone in older age).
The strongest evidence-based conclusion is not that aging has zero effect on male androgens, but that the common narrative of an inevitable, steep, universal testosterone collapse that leads to low testosterone is exaggerated, and that poor health substantially amplifies whatever natural declines do occur.
And since the purpose of TRT is to treat low testosterone, given that low testosterone with age is by no means an inevitability, but rather the consequence of health problems stacked on top of aging, testosterone declines from aging alone do not necessitate treatment with TRT.
Most of the chronic diseases and comorbidities that exaggerate testosterone decline with age are caused by evolutionary mismatches – conditions produced by a modern environment that is fundamentally out of alignment with how humans evolved to live.
Some examples include:
- Sedentary lifestyles
- Processed foods
- Circadian rhythm misalignment
- Chronic stress
- Social isolation
- Environmental toxins & endocrine disrupting chemicals
Therefore, looking at present-day hunter-gatherer populations whose lifestyles are similar to those of our pre-modern forefathers can give us insights into the degree to which testosterone decline with age is a naturally occurring phenomenon versus a byproduct of modern living.
Testosterone Levels & Aging in Hunter-Gatherer Populations

One study, which compared free testosterone levels with age in American men versus three hunter-gatherer style populations, concluded that: "The most important general observation from these data is that age-related declines in free testosterone is not a uniform characteristic of all populations" (10)
Testosterone levels in the hunter-gatherer populations declined significantly less with age than in American men. However, this may be due to the fact that their testosterone levels were lower to begin with, because they have less food availability and more active immune systems (due to higher pathogen exposure), both of which suppress testosterone production.
That said, given that most chronic diseases are virtually non-existent in hunter-gatherer populations, the lower magnitude of testosterone decline observed in these populations probably isn't solely because they have lower levels to begin with, but is also connected to their superior health.
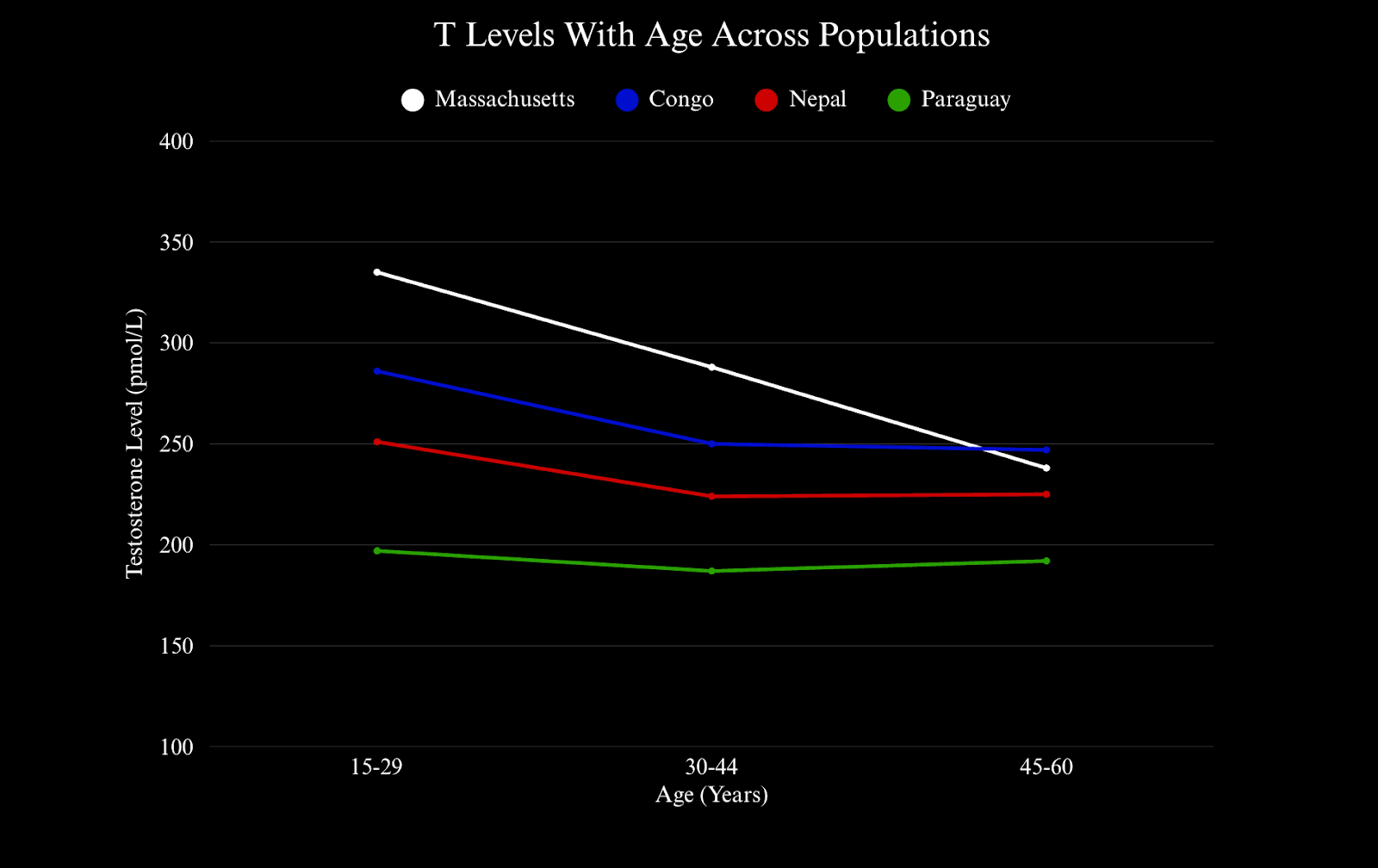
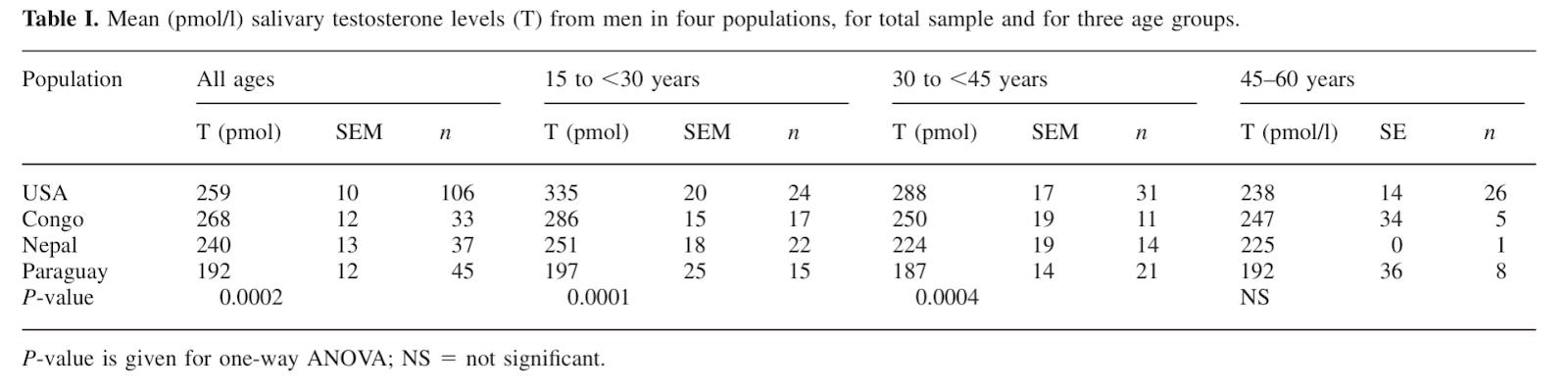
This is an exact visual representation of the study’s findings. I created this figure by plotting the mean testosterone levels from the men in each population at three age groups (15-20, 30-44, 45-60). X axis = age (years). Y axis = testosterone level (pmol/L).
Manual Labor
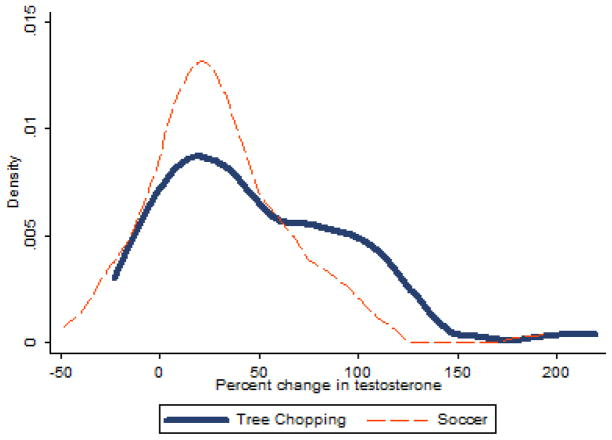
This assertion is supported by another study showing that Tsimane forager-horticulturalists continue engaging in horticultural activity (chopping down and clearing trees) into their eighties, and that testosterone spikes following manual labor were of equal magnitude in all men, regardless of age, unlike in industrialized nations, where older men exhibit blunted post-exercise testosterone spikes in comparison to younger men. (11)
Competition
Another study on the Tsimane found that competition-induced testosterone spikes were equal in magnitude across all ages (16–60). (12)
Reproduction
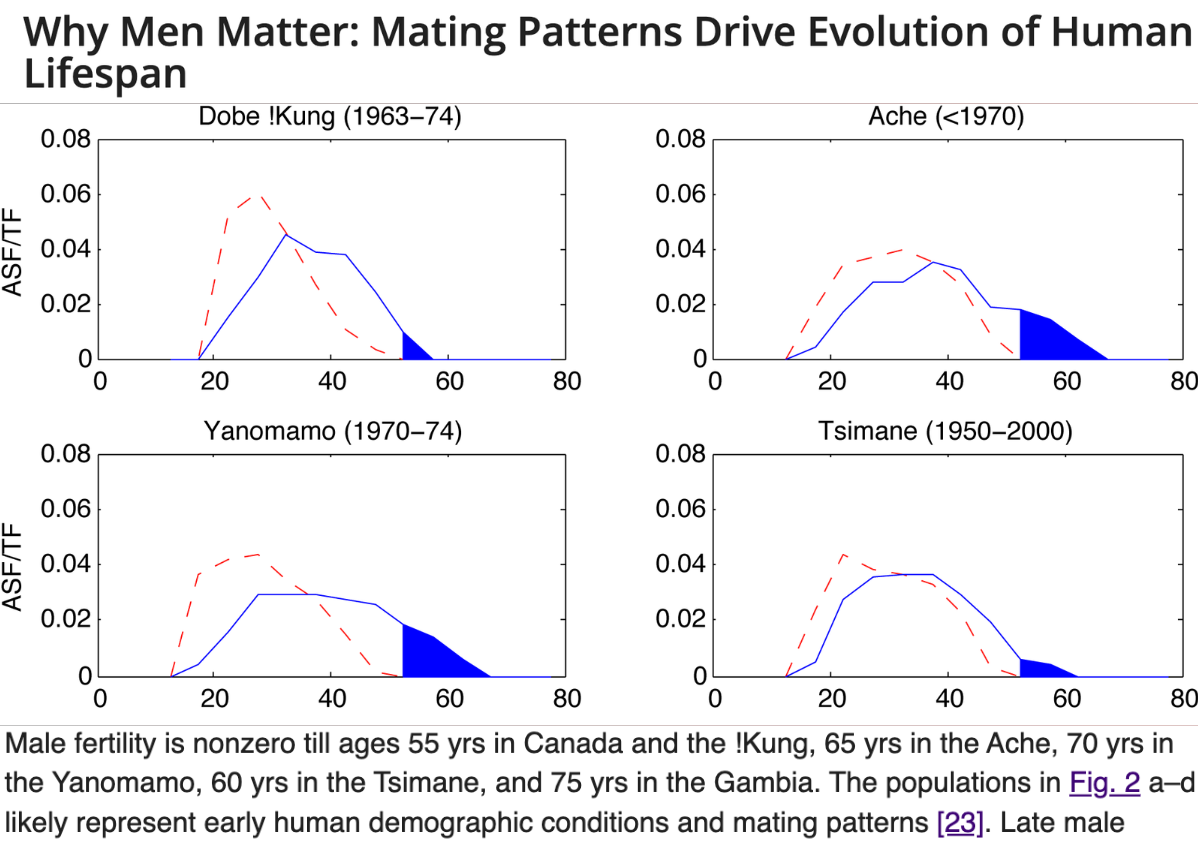
A third study showed that men across four different hunter-gatherer societies continue reproducing up to their early 70s. (13) Testosterone plays a key role in libido, erectile function, and sperm production, so clearly, their levels must be sufficient in order to be capable of reproduction at advanced ages.
How a man feels and performs are the most important indicators of the health of his testosterone levels.
Given that men in hunter-gatherer populations remain engaged in manual labor, competition, and reproduction into their geriatric years shows that their testosterone levels remain adequate with age.
And since the lifestyles of these men emulate those of our evolutionary forefathers, the evident lack of low testosterone in these men provides strong evidence that the prevalence of late-onset hypogonadism seen in industrialized populations is more of a byproduct of evolutionary mismatches in the modern world than a consequence of natural aging.
Men Throughout History Didn’t Need TRT

Further evidence to support this point is that countless male historical figures demonstrated incredible feats of physical prowess, leadership, and accomplishment that would not have been possible had they been burdened by low testosterone symptoms.
Julius Caesar commanded armies at 50. Marcus Aurelius ran an empire and wrote one of the most demanding philosophical works in history at nearly 60 years old. Alexander the Great conquered the known world before 33. Genghis Khan continued fathering children well into his sixties. The list goes on and on.
These men didn't need to inject testosterone to maintain their edge because they were physically capable, high-status, purpose-driven men who strove for greatness until their last breath.
How the Aging Male Body Naturally Compensates for Testosterone Decline
The last point I want to make is that male physiology appears to naturally compensate for age-related testosterone decline by:
- Slightly increasing DHT (8)(3).
- Upregulating LH production (the signal from the brain that tells the testes to produce testosterone) (14).
- Reducing the breakdown rate of testosterone (causing pre-existing testosterone to circulate for longer) (17).
- Retaining the ability to spike testosterone when needed (such as during manual labor and competition) (11).
Putting this all together, we can conclude that:
- Testosterone decline with age is mostly driven by chronic disease.
- Healthy men maintain eugonadal total and free testosterone levels throughout life.
- Late-onset hypogonadism is not observed in hunter-gatherer societies or throughout human history.
- The aging male body compensates for testosterone decline on its own.
All of this provides strong evidence that aging itself does not cause low testosterone, and therefore does not necessitate treatment with TRT.
That said, there are instances where TRT is necessary that are important to delineate before moving forward.
When TRT Is Actually Warranted
When TRT is used to serve its intended purpose – to bring low testosterone levels to the healthy range, it is very safe and effective.
Note that all of the following benefits of TRT are specifically in men with clinically low testosterone, and when TRT is administered at physiologic doses (within the range of what the male body produces naturally).
TRT has been shown to produce marked improvements in body composition, sexual desire and function, bone mineral density, memory and cognition, and red blood cell production (14)(15)(17).
TRT also reduces whole-body oxidative stress (18) – the main cause of most cellular damage and bodily degradation, because testosterone at natural levels is cytoprotective.
According to the literature, TRT use is only warranted when blood testosterone levels are clinically low (hypogonadal) and symptoms are present.
In my opinion, there is one more criterion that should be met before TRT is considered: the cause(s) of low testosterone must be completely out of one's control.
The most pertinent examples of this are severe testicular damage and genetic conditions that lead to low testosterone.
For example, one man who trained at the gym where I was a personal trainer had a brutal case of testicular torsion, and lost most of the functionality of one of his testicles. TRT significantly improved his quality of life.
Another example where TRT use is warranted is in cases of Klinefelter syndrome – a genetic condition where a male is born with an extra X chromosome, which impairs normal androgen production.
Aside from edge cases where low testosterone is completely out of one's control, TRT is not inherently necessary at any age, because all of the other causes of low testosterone can be remediated through lifestyle interventions, which is why…
Why Aging Is Not a Valid Reason to Take TRT
The notion that men need TRT after 40 is predicated on the assumption that low testosterone with age is an inevitability, because the purpose of TRT is to bring low testosterone levels within the normal range.
I want to reiterate that testosterone decline and low testosterone are not the same. While aging does cause some decline, aging alone does not lead to low testosterone. Only when aging is confounded by an unhealthy lifestyle does the risk of low testosterone become more significant.
So unless you have a genetic condition or severe testicular damage, the leading cause of low testosterone with age is poor health.
Despite this, the number of TRT prescriptions has quadrupled (1).
Risks of TRT
Although TRT is generally safe when monitored properly, there are some risk factors, such as prostate enlargement and blood clotting (14)(17). Based on my review of the literature, these risks are pretty rare unless you have a preexisting condition.
But there's one potential risk that I haven't heard anyone else talk about before…
TRT Reverses the Benefits of Natural Testosterone Decline
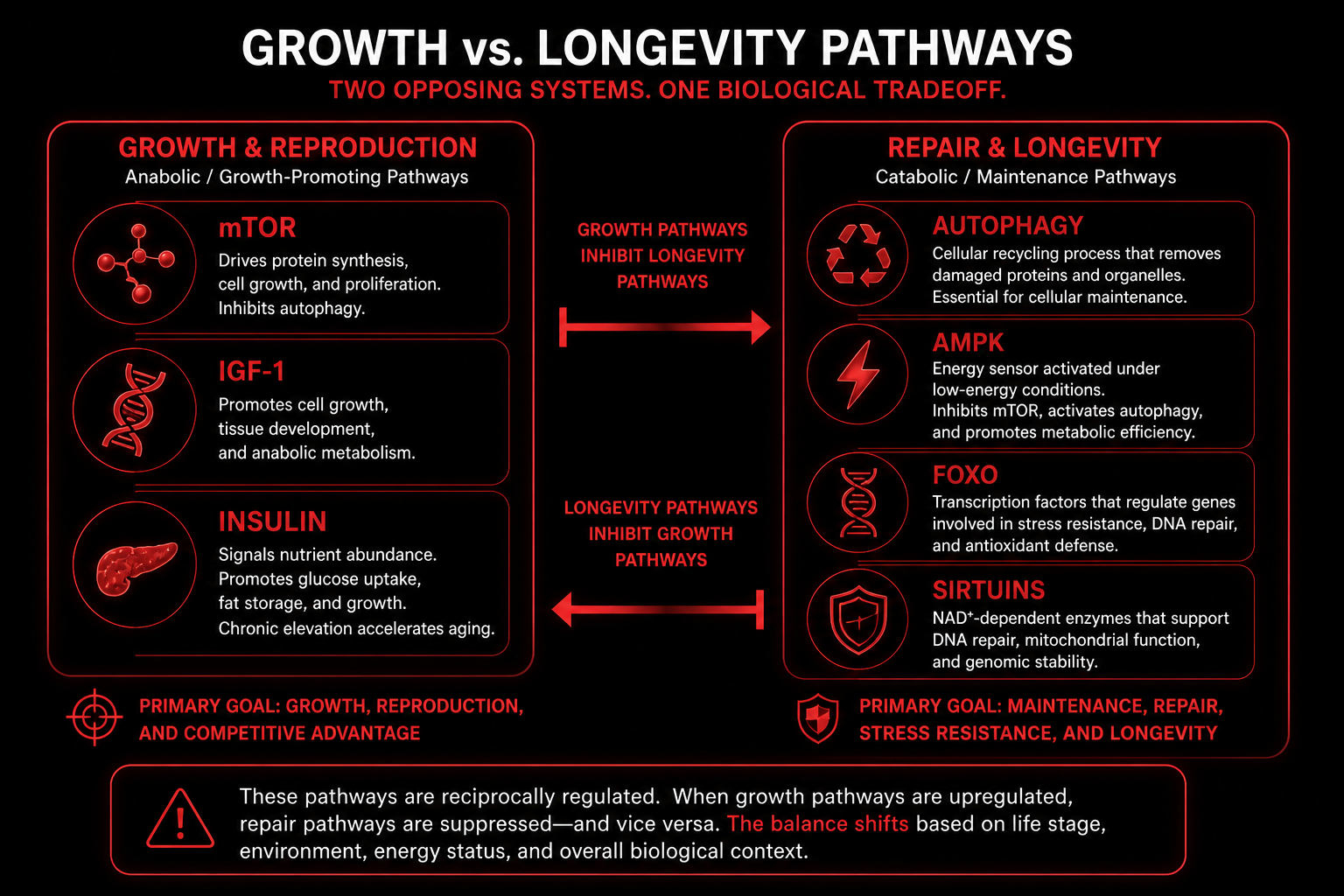
There is a well-established theory in evolutionary biology that there is a tradeoff between longevity and reproduction. Any effort an organism puts into reproduction necessarily comes at the expense of longevity, and vice versa (20).
Testosterone's primary purpose is to encourage reproductive effort.
However, the very features of testosterone that make it encourage reproduction come at the expense of longevity. This is true both physiologically and behaviorally.
Physiologically, testosterone makes a man physically fit to reproduce by increasing metabolism (energy production) and promoting muscle growth.
Cellular metabolism creates some oxidative stress as a natural byproduct. Oxidative stress is thought to be one of the leading causes of biological aging (19).
Moreover, the cellular pathways that drive metabolism and muscle growth are the biological reciprocals of the pathways that drive longevity. Both cannot run at full throttle simultaneously.
Therefore, mild reductions in testosterone with age may be the body's way of shifting its physiological priorities away from reproductive effort toward lifespan extension (20).
It gets confusing in the modern world when subtle, natural declines get exaggerated by poor health to the point where testosterone levels drop to excessively low. Because then, using TRT to bring testosterone levels back up to normal can be beneficial for longevity.
But in cases where testosterone declines slightly in healthy men, and levels stay within the normal range, using TRT to bring their testosterone levels up to those of a 20-year-old might be reversing a process that nature intended.
There's actually a name for this process. It's called somatopause. You can think of somatopause as reverse puberty, because the same hormones that go up during puberty (growth hormone and testosterone) go down during somatopause.
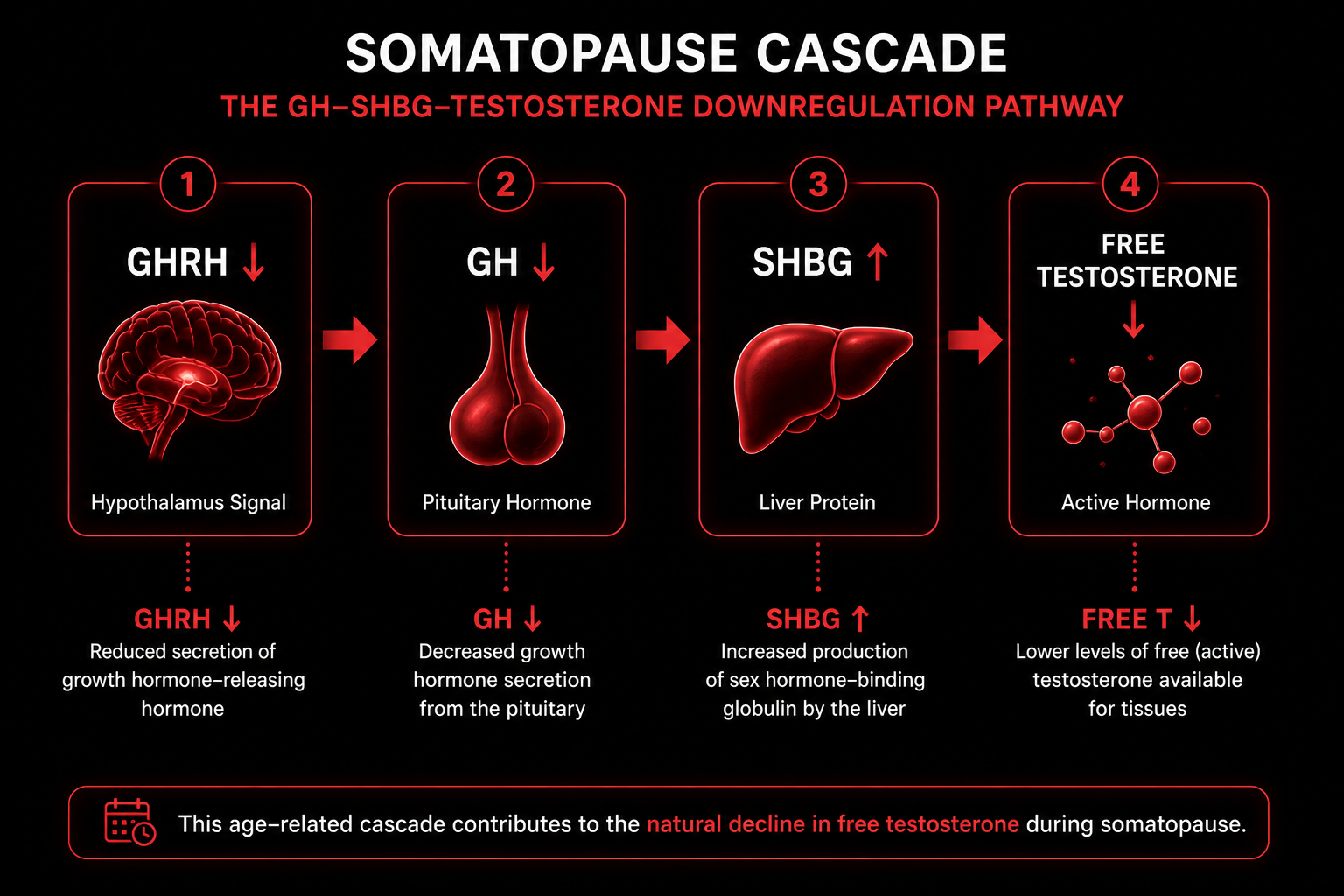
We can all agree that depriving adolescent boys of these hormones would be detrimental to their development.
Could it be that pharmacologically replacing these hormones in healthy aging men could be detrimental to their longevity?
Testosterone also encourages behaviors that promote reproduction, including libido, competition, risk-taking, and physical exertion.
It's plausible that, by reducing aggression and risk-taking in men, natural, age-related testosterone decline could have also evolved as a way to protect men from themselves.
Given its effects on male physiology and behavior, natural testosterone declines with age may have evolved as a mechanism to promote longevity over reproduction.
By taking TRT, and keeping your testosterone levels on the high end of the spectrum when they may be supposed to be on the low-normal end at older ages, you may be artificially negating your body's efforts to extend your lifespan (21).
I have a full article dedicated to why natural testosterone decline with age may actually be a good thing if you're interested in a deeper dive on this particular topic.
Studies have also suggested that "normal" testosterone levels should be stratified by age, meaning what could be considered low for a 30-year-old would actually be healthy for a 70-year-old (16).
Given this, I have concerns with shooting up the entire aging populace with TRT. I don't think a society full of older men with high-range testosterone would necessarily be a good thing, not only for their longevity but also for the psychosocial dynamics of society.
Because slightly lower (but not low) testosterone causes men to be more reflective and deliberative. This is a case where more testosterone doesn't always equal better. The yin of older men to balance the yang of younger men is important to preserve.
In my view, what we need to do is this: minimize excessive, artificial declines in testosterone caused by poor health and modern living, but after that, leave natural declines alone, as long as they don't lead to negative low testosterone symptoms. At that point, TRT can be considered, but only if the man is already exhausting lifestyle interventions.
The most impactful and proven side effect of TRT that men need to be aware of is that TRT makes you infertile while you're on it.
TRT Suppresses Fertility
TRT causes infertility by shutting down natural testosterone production.
This happens because the body (specifically, a gland in your brain called the hypothalamus) constantly gauges how much testosterone is circulating in the bloodstream, because in biology, too much or too little of anything becomes harmful. The body always wants to maintain homeostasis – keeping all systems in a Goldilocks zone.
When testosterone levels drop too low, the hypothalamus sends signals (Luteinizing Hormone, or LH) to the testes to increase testosterone production.
When testosterone levels rise too high, the hypothalamus secretes less LH, leading to less testosterone production downstream.
When a man injects TRT, his body is deceived into "believing" that it's already producing plenty of testosterone, so it stops producing its own.
This causes infertility because testosterone is a key driver of sperm production. Without testosterone, sperm production cannot be complete (22).
But here's the kicker. Only testosterone that's produced from within the testes themselves is capable of supporting sperm production (termed "intratesticular" testosterone) (22).
This is because the barrier between the testes and the rest of the general blood circulation is a one-way street – testosterone can only exit the testes, it cannot enter them (22).
Therefore, TRT, which is injected into the bloodstream, cannot enter the testes to support sperm production. The end result is that TRT shuts down the intratesticular testosterone that's needed to drive sperm production, but is incapable of supporting sperm production itself (22).
Can You Preserve Fertility on TRT?
TRT-induced fertility loss only occurs while on TRT and is reversible in most cases. Research shows that 90% of patients return to baseline sperm concentration values after one year of TRT cessation, and 100% after two years (22).
Nonetheless, the guidelines in the World Journal of Men's Health explicitly state that: "if a patient currently desires fertility, TRT should be avoided or discontinued immediately," and "the recovery of spermatogenesis is unclear for patients on chronic TRT" (22).
Despite this, one survey revealed that 25% of urologists (doctors who specialize in male reproductive health) reported that they would use TRT to promote sperm production in infertile men, which is completely paradoxical because TRT suppresses fertility (23).
hCG has been shown to be effective in preserving sperm production in men on TRT for up to one year, (23) however, its efficacy appears to be partly contingent on the health of the user.
One study reported that: "hCG treatment was not equally effective in all men. Individual response to treatment is likely influenced by genetic variability and overall health status" (24).
Since low testosterone is caused by poor health, the type of man who would need TRT in the first place is the exact archetype who would be at the highest risk of fertility complications coming off of TRT.
So even if TRT-induced infertility can be prevented with hCG or recovered after TRT is stopped, the deepest problem with TRT is that it leaves the underlying causes of low testosterone unaddressed, and those same causes of low testosterone can lead to subfertility.
If you're interested in having children at some point in the foreseeable future, understand that TRT will shut down your fertility while you're on it (unless you take hCG along with it), and more importantly, TRT just masks the symptoms without addressing the root causes, which will still be there to squander your fertility whether or not you're taking TRT.
Fertility aside, there are other problems with taking TRT unnecessarily, which I defined as using TRT when low testosterone could be corrected naturally.
Joe's Story: What Happens When Men Take TRT When They Don’t Actually Need It
I'm going to illustrate the consequences of taking TRT unnecessarily with the story of a man we'll call "Joe" – a 42-year-old father and software developer who told me that he'd been on TRT for nearly two years.
As I asked more questions about his lifestyle, it became more and more apparent why he had low testosterone.
- Joe had a gastric bypass that helped him lose 50 pounds, but he was still walking around at 27% body fat (obese).
- Joe was type II diabetic.
- He only exercised for 30 minutes twice per week.
- His dietary staples were Dunkin breakfast sandwiches, protein bars, and salad.
- He averaged 4–5 hours of sleep per night.
- He reported being chronically stressed but did nothing to manage it.
- He recently went through a divorce and was let go from his last job (a study on testosterone decline with age found that both loss of spouse and loss of employment decreased testosterone as much as obesity) (9).
All of the above are direct contributors to low testosterone that can be corrected without TRT.
Joe reported that TRT helped slightly with fat loss and muscle gain, but the main benefit he noticed was improved energy and less fatigue.
Joe’s goals were to be physically fit and capable for his future children.
When I asked him if he was aware that TRT suppresses fertility, he said that he was taking hCG so he “should be fine.” But here’s the thing.
All of Joe’s underlying health problems reduce the efficacy of hCG, and are also risk factors for poor sperm quality and male factor infertility.
So even if hCG did prevent fertility loss, Joe’s reproductive system was still being assailed by all of his unhealthy lifestyle habits listed above.
Not to mention that those same unhealthy habits are also risk factors for virtually every other chronic disease (heart disease, cancer, neurodegenerative disease, etc).
To make matters worse, taking TRT actually removed the incentive for Joe to correct his unhealthy habits that were causing his health problems.
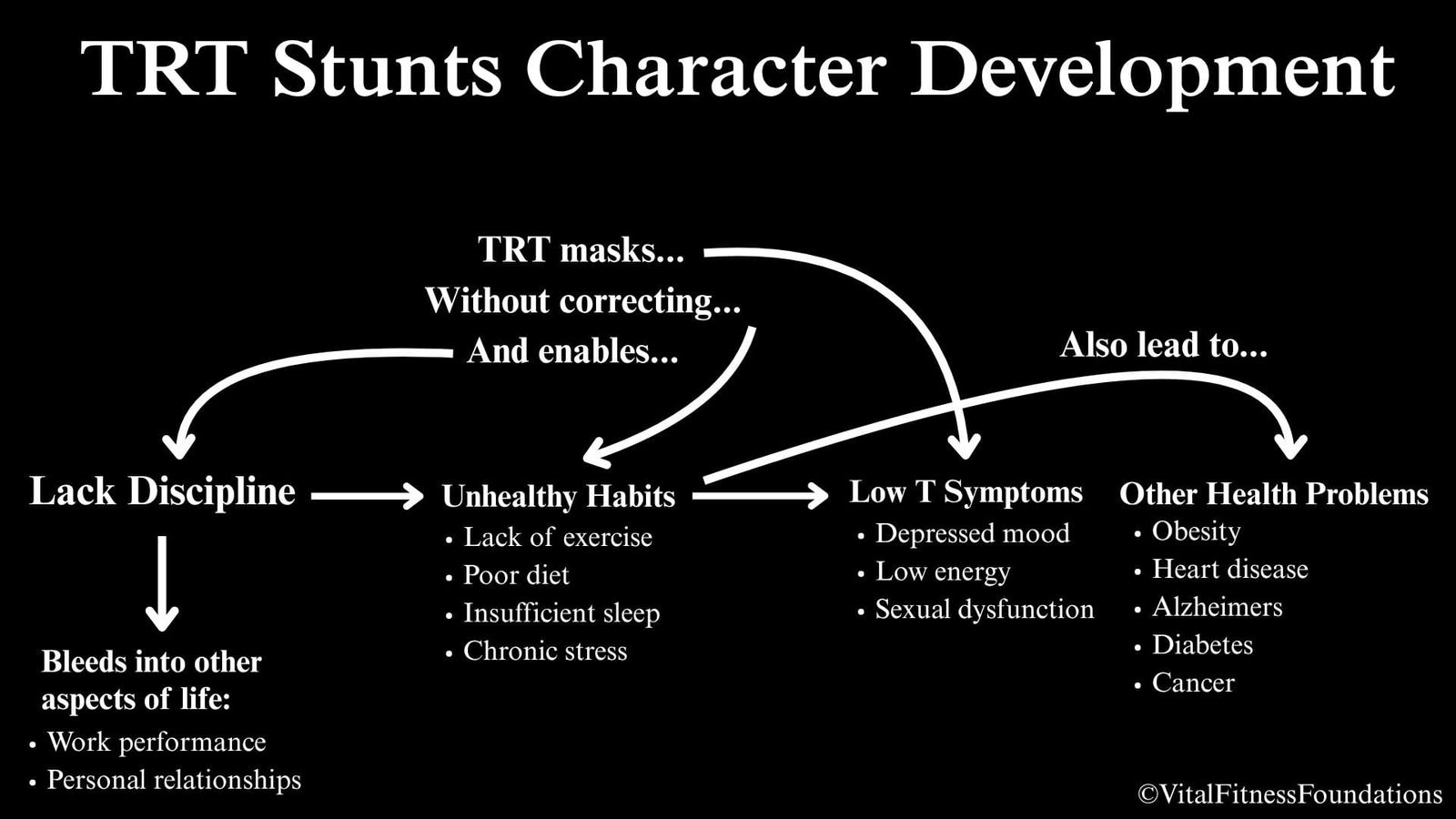
TRT Enables Unhealthy Habits
According to Sigmund Freud’s pleasure and pain principle, humans only take action when the pain of inaction outweighs the effort of action.
I vividly remember Joe saying something along the lines of “why would I try to get more sleep when the TRT gives me energy?”
Insidiously, by improving his low energy and chronic fatigue for him, TRT removed the pain that would have otherwise prompted Joe to fix his sleep, which was one of the primary causes of his low testosterone.
Morals of the story:
- TRT is not a magic bullet. Joe still wasn’t anywhere near his fitness goals.
- TRT did not address Joe’s unhealthy lifestyle habits, which were causing low testosterone and increased his risk of infertility and every other chronic disease.
- TRT enabled Joe’s unhealthy lifestyle habits by removing the felt consequences of them.
So even though TRT brought Joe’s testosterone levels up to "normal" on paper, on the inside, he was still just as unhealthy as he was before he started TRT.
Worst of all, Joe didn’t even need TRT. He could have reversed all of his health problems: low testosterone, obesity, and diabetes – by correcting his unhealthy lifestyle – lack of sleep and exercise, poor diet, and unmanaged stress.
Taking TRT instead of correcting lifestyle doesn’t just worsen a man’s physical health – it also weakens his character.
The Deepest Root Cause of Low Testosterone
We’ve established that the root cause of Joe’s low testosterone was his unhealthy lifestyle. Going one level deeper, the root of Joe’s unhealthy lifestyle habits stemmed from a lack of something called executive function. For example:
- Making an effort to learn why one’s health is suffering requires cognitive exertion.
- Exercise requires the discipline to endure discomfort (“pain”).
- Eating clean requires inhibitory self-control to refrain from unhealthy food (“pleasure”).
- Staying consistent and not giving up when results don’t come immediately require delayed gratification and foresight.
- The ability to make exercise, sleep, and a healthy diet priorities requires prioritization and time management,
- Stress management requires self-awareness, introspection, and emotional regulation.
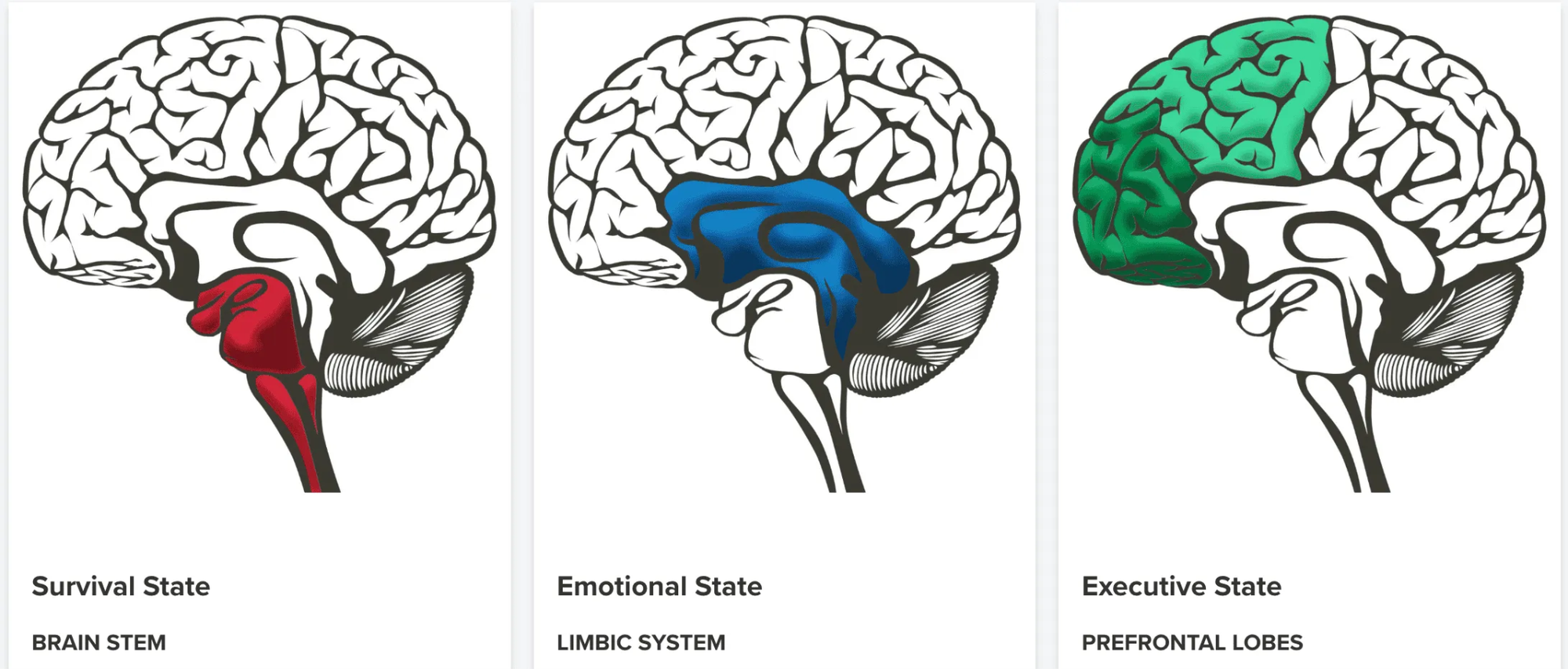
All of the bolded skills listed above fall under the umbrella of executive function – a set of mental skills governed by the brain's prefrontal cortex that make it possible to set goals, manage emotions, and execute tasks.
Since low testosterone is caused by unhealthy lifestyle habits, and unhealthy lifestyle habits are caused by a lack of executive function, the deepest root cause of low testosterone is a lack of executive function.
TRT Undermines Executive Function
Executive function is controlled by the most evolved part of the brain – the prefrontal cortex.
In contrast, the part of the brain that causes us to avoid exertion and discomfort, drives us toward pleasure, and creates emotions is called the limbic brain.
The limbic brain used to be great for survival throughout our evolution because it:
- Drove us away from the “pain” of exertion (burning extra calories) and discomfort (hunger, heat, cold, etc).
- Drove us toward the “pleasure” of eating and reproducing.
- Scared us away from danger (predators, other hostile humans, etc).
As humans evolved and become more advanced, we have become less limbic dominant and increasingly prefrontal cortex dominant, because the prefrontal cortex armed us with higher intelligence and the ability to cooperate – the competitive advantages that made humans the most dominant species that ever existed.
The “problem” in the modern world is that the advancement of our outer environment has outpaced the evolution of our brains and bodies.
Even though our physical safety and survival are safeguarded by modern advancements, our limbic brains still tell us to take the path of least resistance and most pleasure, and to be hypervigilant to threats, causing us to be sedentary, gluttonous, stressed, and anxious.
The good news is that the prefrontal cortex has the ability to exert what’s called “top-down” control over the limbic brain. In other words, when the prefrontal cortex is “strengthened” through repeated use, it can override the limbic brain.
The next stage of human evolution will involve exercising this capacity for top-down control so that we can make decisions that are good for ourselves and others.
On the individual level, this looks like making healthy food choices, choosing to stay active, and managing fears and stress, so that we can remain physically healthy enough to live long lives.
But when drugs like TRT remove the pain (i.e. low testosterone symptoms) of failing to make good health decisions, the lesson is never learned and the lack of executive function remains.
In Joe’s case, by always trying to take the easy way out, whether that be a gastric bypass for obesity, or TRT for low testosterone, he was unknowingly weakening his prefrontal cortex.
Beyond his own physical health, Joe’s lack of executive function seemed to have a negative ripple effect on those around him and society at large.
In life, how you do anything is how you do everything.
I’m willing to infer that Joe’s habit of taking the easy way out of everything also contributed to his divorce and being let go from his job.
So not only do drugs like TRT enable a lack of executive function that negatively affects the health and wellbeing of individuals, but that same lack of executive function bleeds into the rest of society.
How Overcoming Low Testosterone Naturally Changed the Trajectory of My Life
In my early 20’s I struggled with a number of health problems:
- Erectile dysfunction
- High blood pressure
- Heart arrhythmia
- Chronic stress & anxiety
- Probable low testosterone
Because of my unhealthy lifestyle:
- A dining hall diet and dorm room snacks
- Alcohol and marijuana use multiple times per week
- Staying out late partying instead of getting enough sleep
- Habitual porn and masturbation
- Lack of stress management skills
- 17% body fat

Side note: my story goes to show that low testosterone can afflict a man at any age, including when testosterone is “supposed” to peak.
On the flipside, an older man in excellent health could be biologically “younger” than a younger man in poor health, with higher testosterone levels to show for it.
This is because a man’s testosterone levels are reflective of his biological age, which is based on how well cells function, not his chronological age (the number of years he’s been alive).
Back to the story.
On the outside, I was a straight A student and 3X college football champion, but on the inside I was stressed, anxious, and unconfident. I covered it all up by distracting myself with pleasure and what I thought would get me approval from my peers.
After multiple embarrassing sexual encounters, repeated panic attacks from heart flutters, and workload burnout every semester, I had enough.
Why I Refused Drugs And What I Did Instead
My doctor was utterly useless.
I was offered:
- Lisinopril for my blood pressure
- SSRIs for my stress & anxiety
- Viagra for my erectile dysfunction
- Beta blockers for my arrhythmia
Refusing to spend the rest of my life on drugs, I kindly declined and took matters into my own hands.
I leveraged the strongest executive function I had at the time, my ability to learn and study, and spent the ensuing months devouring books, studies, podcasts, and articles on men's health.
I even added Biology as a second major on top of Exercise Science in part to augment my scientific literacy and deepen my understanding of the mechanisms behind what was going on with me.
After being enlightened to the fact that sub-optimal testosterone was the root cause of all of my problems…
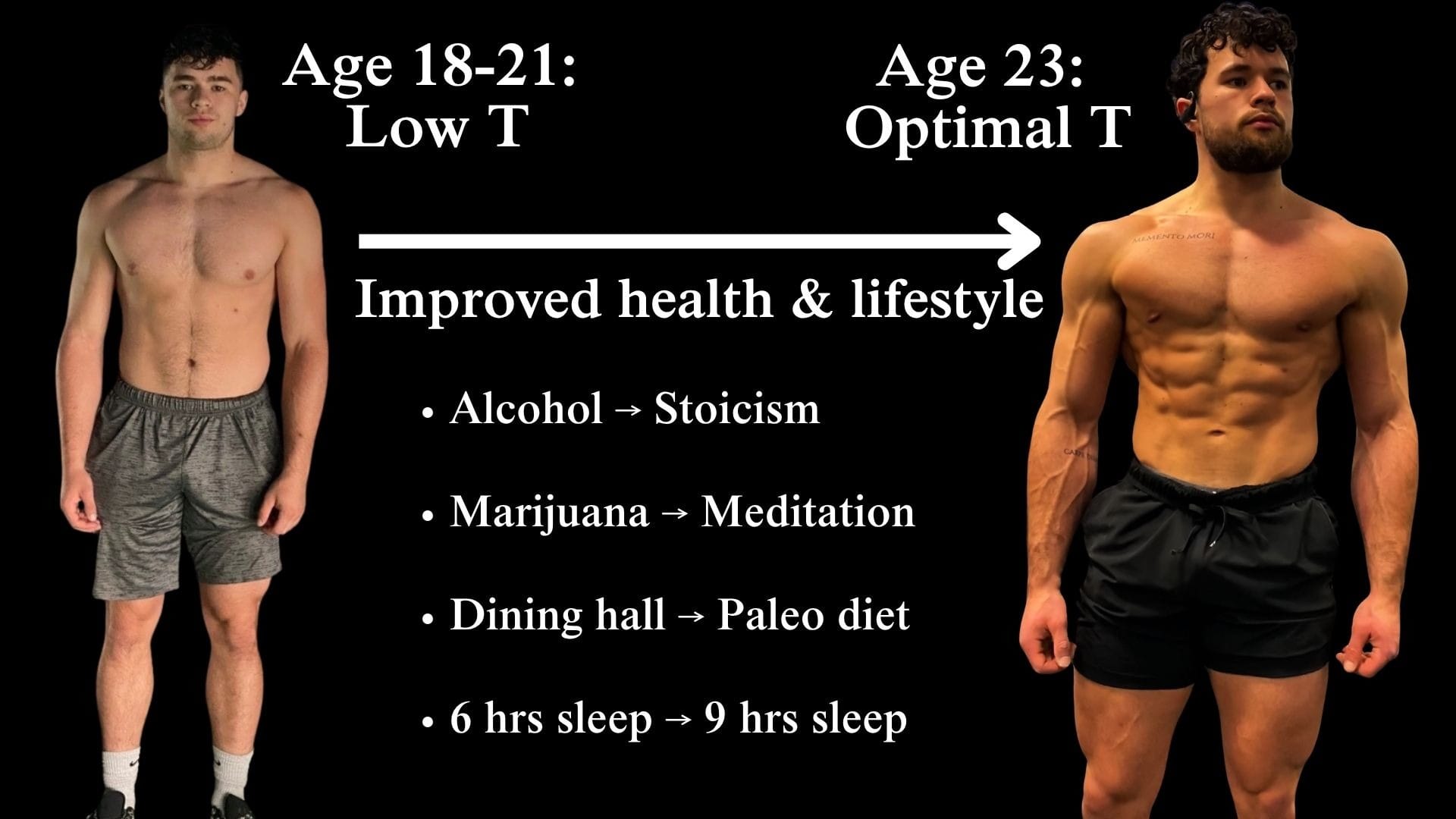
- I stopped drinking and smoking.
- I cleaned up my diet.
- I made sleep a top priority.
- I quit porn and masturbation.
- I started meditating, reading stoic philosophy, and journaling.
After consistently implementing these changes for several months:
- My blood pressure dropped from 150/90 to 110/80.
- My erections returned with vengeance.
- My mind was calm and capable of coping with any challenge life threw at me.
- My physique became unrecognizable, even though my training didn’t change.
My transformation was so life-changing that I spent my entire senior year writing an award-winning thesis on the causes of testosterone decline in our society.
And now, I’ve dedicated my life to using all that I’ve learned, and continue to learn, to help other men overcome low testosterone through my signature coaching program, The Testosterone Transformation Academy.
The moral of my story in the context of this article is that, if you injected the 20 year old version of me with TRT, I wouldn’t have needed exercise my executive function to educate myself on what was going wrong with me, or execute on making the changes necessary to solve my problems once I learned what was causing them.
In other words, if TRT had done the work for me, sure, the end result would have been the same – optimal testosterone and no low testosterone symptoms – but I would have never developed my executive function by going through the process of overcoming my challenges on my own.
For example, I actually tried Viagra, but it didn’t work for me because I didn’t have a blood flow problem, I had a nervous system regulation problem.
I didn’t realize it at the time, but the same performance anxiety that showed up during sex showed up in other areas of life:
- On the football field, I was a great athlete, but overthinking held me back.
- In my academics, I studied rigorously and knew the material well, but would get nervous before exams and presentations, which hampered my ability to access what I learned when I needed it the most.
To this day, I’m grateful that Viagra didn’t work, because I ended up buying a course on overcoming psychogenic ED, and the main focus was nervous system regulation and performance anxiety management.
The skills I developed in that course not only helped me overcome ED, but also transferred to my athletics and academics.
That course was also the gateway to my discovery of stoicism and meditation – both of which have drastically improved my resilience, decreased my perceived stress, and improved my mental health, which had the ancillary health benefits of lowering my blood pressure and cortisol, and thereby increasing my testosterone.
If Viagra did work, I wouldn’t have bothered to learn how to regulate my nervous system, and I could've died early from a heart attack.
Although I didn’t realize it, my health challenges were among the best things that ever happened to me, because as Marcus Aurelius said: “The impediment to action advances action, what stands in the way becomes the way.”
What stood in my way at the time – my health problems – advanced my action to become a stronger version of myself and became the way through which I discovered my calling in life.
If I had taken drugs to solve my problems instead of developing the executive function to overcome them, the ripple effects would have extended well beyond my own life and into society at large.
How Overcoming Low Testosterone Naturally Changed the Lives of Others
Without the process of overcoming my physical and mental health challenges and viscerally feeling the profound transformation in my quality, I wouldn’t have developed my obsessive passion for men’s health.
I wouldn’t have had the conviction to walk away from a conventional medical career to build a business that actually helps men.
And I wouldn't have had the discipline to do so effectively, because that discipline was forged in the same crucible as my health.
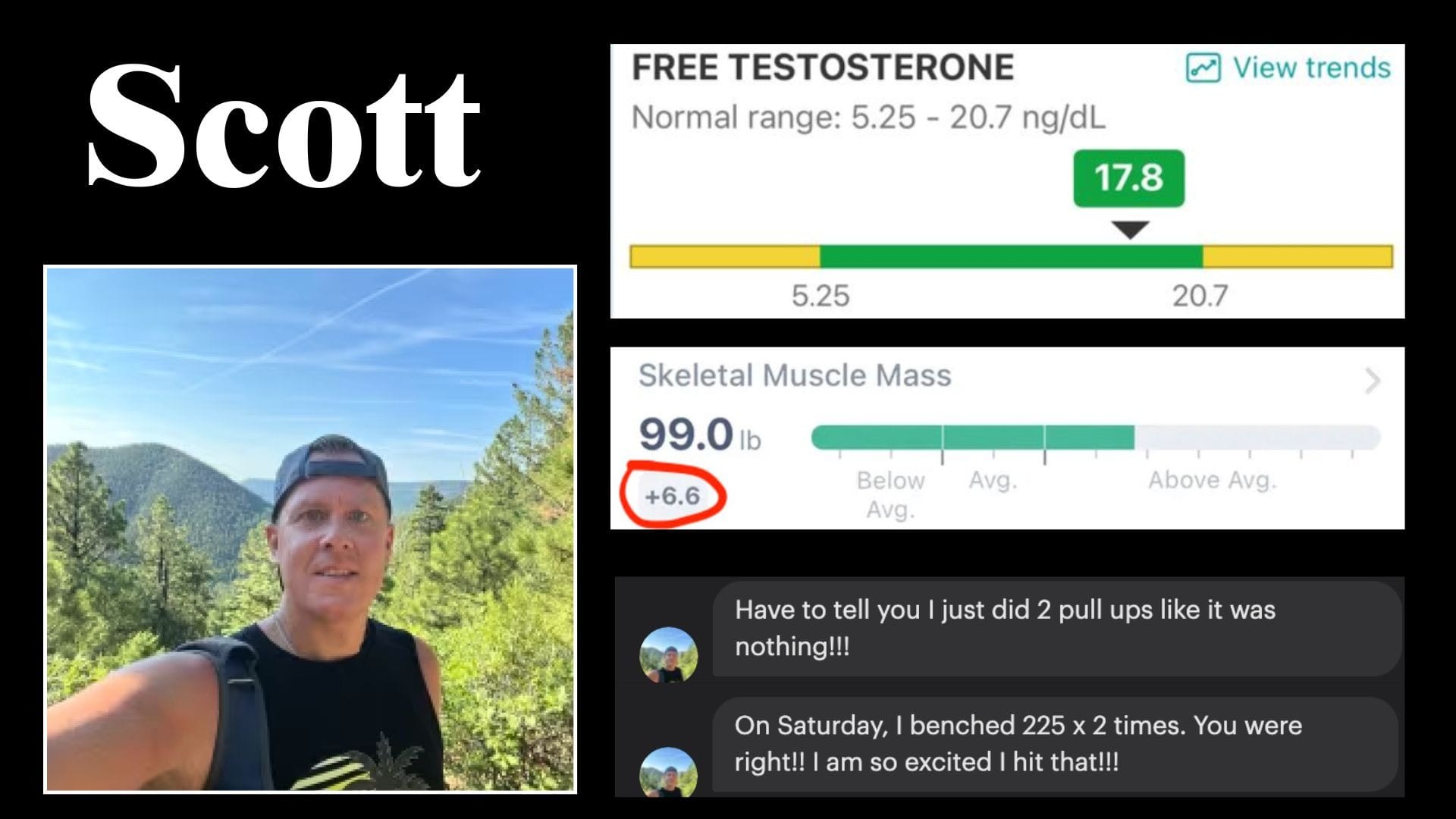
Scott
Father of two, brought his testosterone to the high-normal range at 45, naturally.
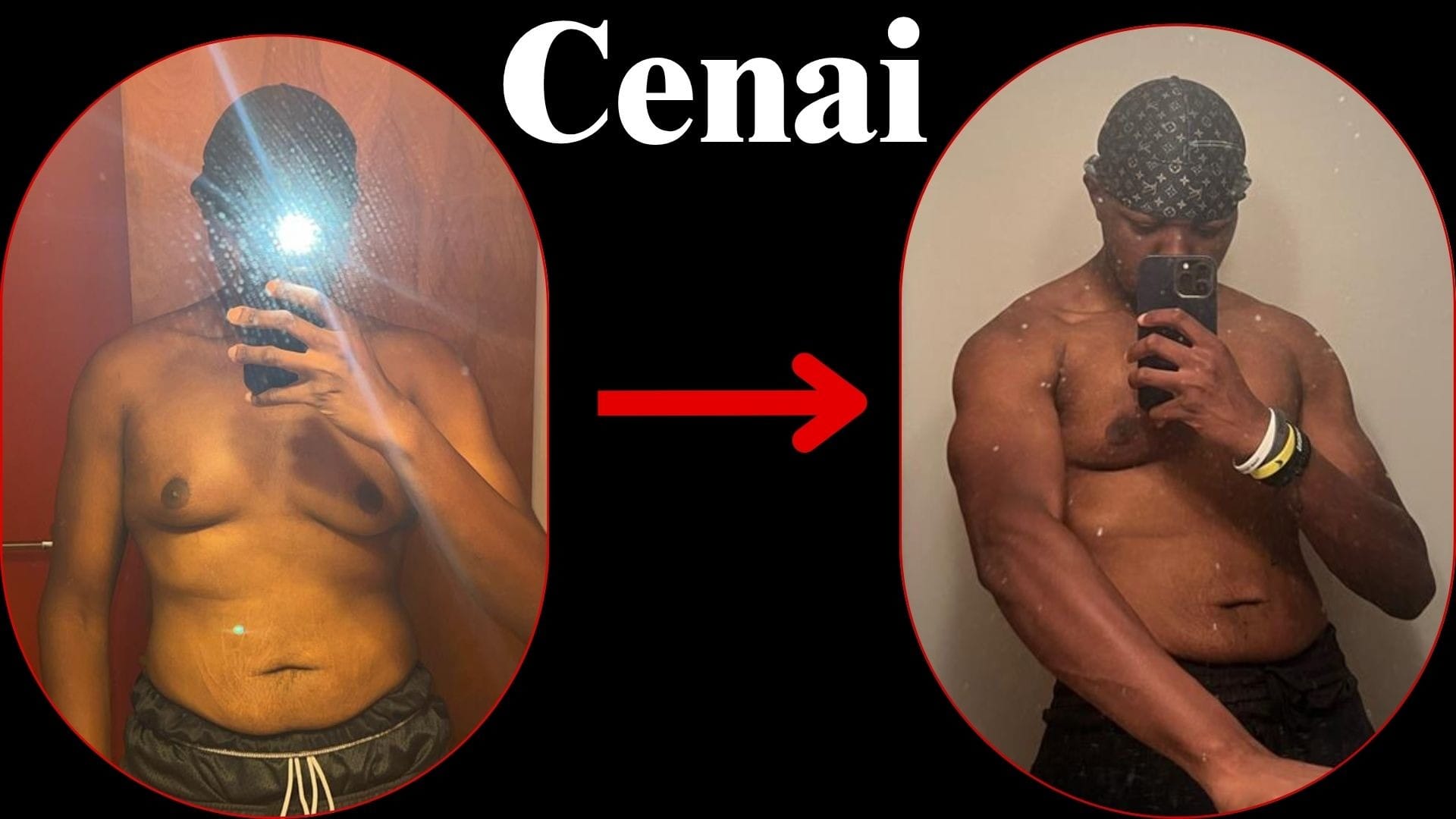
Cenai
Lost 30 pounds, cleared his brain fog, and built the confidence to launch a successful podcast and personal brand.
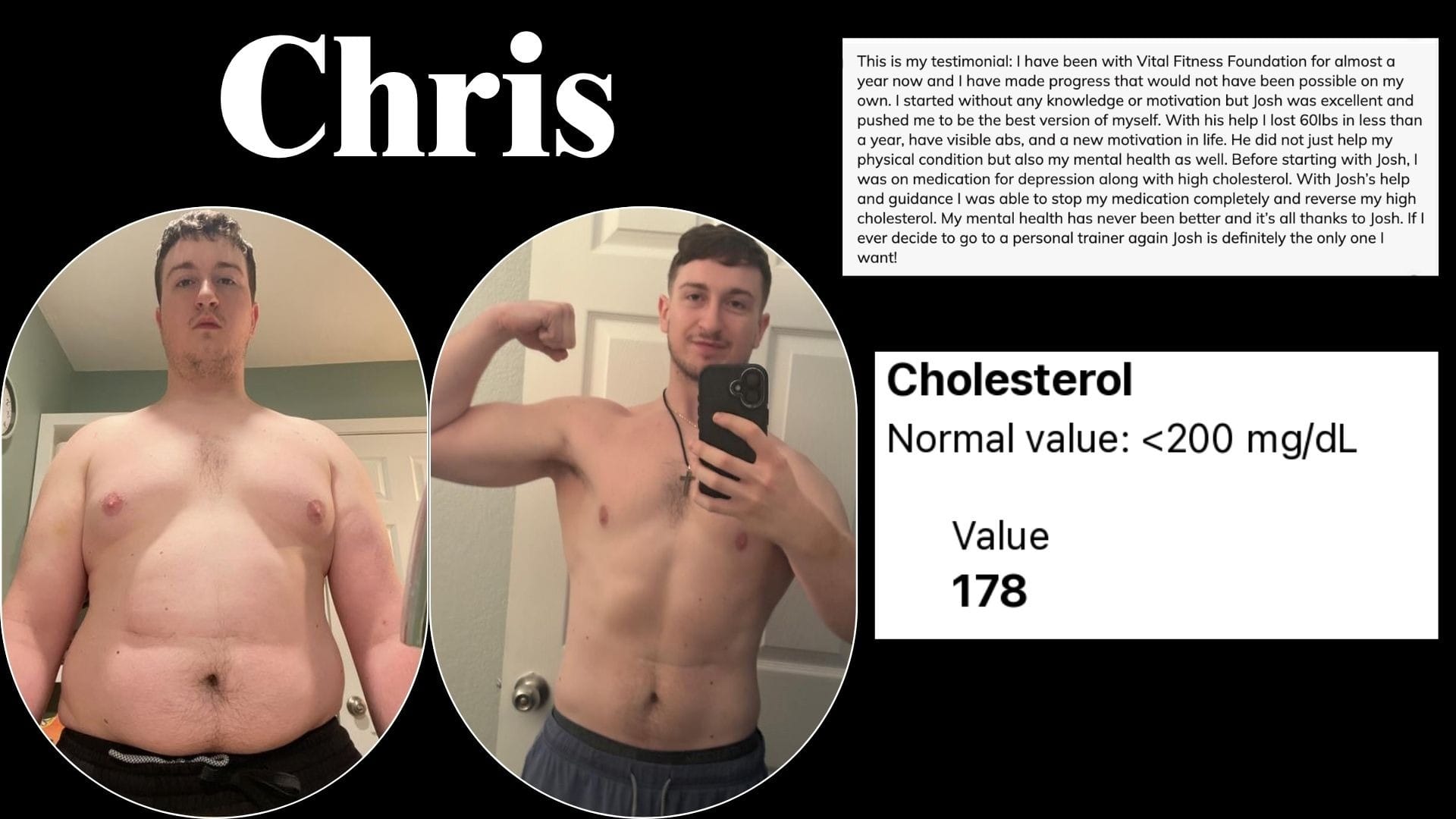
Chris
Lost sixty pounds, came off SSRIs and statins for good, and found his calling in the medical field.
None of their transformations exist if I took the shortcut.
And none of those men would have become more disciplined and confident along the way, because that's what earning your results does that TRT cannot.
TRT Takes Your Confidence
Discipline can be defined as following through on your word.
When you keep your word to yourself enough times, whether it be going to the gym, sticking to your diet, cutting out alcohol, etc, your subconscious trusts that when your prefrontal cortex makes a decision to do something, you do it.
That self-trust is the breeding ground of confidence.
But if TRT does the work for you, no amount of muscle gain, fat loss, or libido the TRT gives you will make you genuinely confident, because your subconscious knows that you didn’t actually achieve the result. TRT did.
Since no self-trust was developed, no confidence was earned.
Every time you inject yourself, you’ll be reminded of your dependency on a needle just to feel like a man.
Taking TRT when you don’t actually need it also robs you of a golden opportunity to develop your executive skills through the process of overhauling your unhealthy lifestyle habits, which is a major problem because if humans are to continue evolving, that’s precisely the skill we need to develop.
Because aside from an interstellar disaster, the only threats to the continuation of life as we know it are consequent to a lack of executive function:
- Chronic disease – inability to resist pleasure and overcome discomfort.
- Climate change – lack of foresight.
- Nuclear arms race – lack of foresight.
- COVID pandemic – tribalism and emotional panic.
To be clear, I’m not insinuating that TRT or other drugs directly brought about these issues.
My point is that, when taken in lieu of lifestyle change, drugs can negate the need to develop executive function, which, when lacking, is what causes most of humanity’s problems.
Executive function is powered by the prefrontal cortex – the exact brain region that enabled humans to out-compete all other life forms as the preeminent species on planet earth.
Thus, when used on a mass scale, drugs that mask the consequences of undisciplined living are contributing to the de-evolution of our species.
But every man who chooses to develop his executive function instead of medicating over its absence is, in a small but real way, part of the solution.
The Alternative to TRT
The alternative to TRT isn't a supplement stack or a biohacking protocol. It's something far simpler and far older: living in a way that's consistent with how your biology was actually built to function.
I call this evolutionary medicine, and it's the entire foundation of my approach to testosterone optimization.
The short version is this: men in modern hunter-gatherer populations maintain healthy testosterone levels well into old age because their daily lives align with the conditions human biology evolved under. They move their bodies, eat real food, sleep in sync with natural light cycles, maintain close social bonds, compete, and contribute to their communities with purpose until the day they die. Low testosterone is virtually non-existent in these men.
Part 5 of this series is a complete breakdown of how to reverse-engineer that lifestyle into a practical protocol for men living in the modern world. It covers body composition, nutrition, sleep, stress, exercise, and the life circumstances that affect testosterone most in older men.
If you haven't read it yet, that's your starting point.
The path exists. It has been walked by every man throughout history who maintained his vitality without a prescription. The only question is whether you're willing to walk it.
Hercules at The Crossroads
There is an ancient Greek parable called Hercules at the crossroads, wherein the great hero Hercules is walking down the metaphorical “path” of life, and arrives at a fork in the road. Each direction is guarded by a goddess.
One goddess, named Kakia (who represents Vice), promised Hercules a life of ease and immediate gratification, free from hardship and struggle.
The other goddess, Arete (who represents Virtue), offered a path of toil, sacrifice, and perseverance. This path would be difficult and fraught with challenges, it would lead to true glory, respect, and lasting fulfillment, and it would bring out the best in Hercules.
Hercules decided to follow Arete’s path of Virtue, which set the stage for his legendary life because in that moment he committed to a life defined by effort, personal development, and purpose, giving rise to all of his victories that followed.
The moral of this parable is that true fulfillment and glory are earned, not given.
If you choose to take TRT to cure low testosterone for you, when it’s fully within your power to do so through self-education and discipline, you are choosing to weaken your character.
On the flipside, if you decide to overcome low testosterone naturally, by cultivating the self-agency to live a physically and mentally healthy life, it will be more challenging, but you will grow physically and mentally stronger, and will be genuinely proud of your results because deep down you know you earned them.
If the second path is more appealing to you, you’re exactly the type of man who would succeed in the The Testosterone Transformation Academy – a men’s health coaching program I’ve developed to help men optimize their testosterone levels naturally.
And don't mistake consulting a mentor for choosing the easy route.
You’re a busy man with a full life. It makes all the sense in the world to bring in an expert who has spent a decade studying this.
Not to do the work for you, but to make sure the effort you put in goes in the right direction.
As the great Marcus Aurelius said "Don't be ashamed to need help. Like a soldier storming a wall, you have a mission to accomplish. And if you’ve been wounded and need a comrade to pull you up? So what?"
References
- Yabluchanskiy, A., & Tsitouras, P. D. (2019). Is testosterone replacement therapy in older men effective and safe? Drugs & Aging, 36(11), 981–989. https://doi.org/10.1007/s40266-019-00716-2
- Muehlenbein, M. P., Gassen, J., Shattuck, E. C., & Sparks, C. S. (2022). Lower testosterone levels are associated with higher risk of death in men. Evolution, Medicine, and Public Health, 11(1), 30–40. https://doi.org/10.1093/emph/eoac044
- Feldman, H. A., Longcope, C., Derby, C. A., Johannes, C. B., Araujo, A. B., Coviello, A. D., Bremner, W. J., & McKinlay, J. B. (2002). Age trends in the level of serum testosterone and other hormones in middle-aged men: Longitudinal results from the Massachusetts Male Aging Study. The Journal of Clinical Endocrinology & Metabolism, 87(2), 589–598. https://doi.org/10.1210/jcem.87.2.8201
- Harman, S. M., Metter, E. J., Tobin, J. D., Pearson, J., & Blackman, M. R. (2001). Longitudinal effects of aging on serum total and free testosterone levels in healthy men. The Journal of Clinical Endocrinology & Metabolism, 86(2), 724–731. https://doi.org/10.1210/jcem.86.2.7219
- Handelsman, D. J. (2016). Age-specific male reference ranges for circulating testosterone. Annals of Clinical Biochemistry, 53(2), 264–272. https://doi.org/10.1177/0004563215610589
- Fabbri, E., An, Y., Gonzalez-Freire, M., Zoli, M., Maggio, M., Studenski, S. A., Egan, J. M., Chia, C. W., & Ferrucci, L. (2016). Testosterone trajectories and reference ranges in a large longitudinal sample of male older adults. The Journals of Gerontology: Series A, 71(11), 1481–1487. https://doi.org/10.1093/gerona/glw021
- Kelsey, T. W., Li, L. Q., Mitchell, R. T., Whelan, A., Anderson, R. A., & Wallace, W. H. (2014). A validated age-related normative model for male total testosterone shows increasing variance but no decline after age 40 years. PLOS ONE, 9(10), e109346. https://doi.org/10.1371/journal.pone.0109346
- Sartorius, G., Spasevska, S., Idan, A., Turner, L., Forbes, E., Zamojska, A., Allan, C. A., Ly, L. P., Conway, A. J., McLachlan, R. I., & Handelsman, D. J. (2012). Serum testosterone, dihydrotestosterone and estradiol concentrations in older men self-reporting very good health: The healthy man study. Clinical Endocrinology, 77(5), 755–763. https://doi.org/10.1111/j.1365-2265.2012.04432.x
- Travison, T. G., Araujo, A. B., Kupelian, V., O'Donnell, A. B., & McKinlay, J. B. (2007). The relative contributions of aging, health, and lifestyle factors to serum testosterone decline in men. The Journal of Clinical Endocrinology & Metabolism, 92(2), 549–555. https://doi.org/10.1210/jc.2006-1859
- Ellison, P. T., Bribiescas, R. G., Bentley, G. R., Campbell, B. C., Lipson, S. F., Panter-Brick, C., & Hill, K. (2002). Population variation in age-related decline in male salivary testosterone. Human Reproduction, 17(12), 3251–3253. https://doi.org/10.1093/humrep/17.12.3251
- Trumble, B. C., Cummings, D. K., O'Connor, K. A., Holman, D. J., Smith, E. A., Gurven, M., & Kaplan, H. S. (2013). Age-independent increases in male salivary testosterone during horticultural activity among Tsimane forager-farmers. Evolution and Human Behavior, 34(5), 350–357. https://doi.org/10.1016/j.evolhumbehav.2013.06.002
- Trumble, B. C., Cummings, D., von Rueden, C., O'Connor, K. A., Smith, E. A., Gurven, M., & Kaplan, H. (2012). Physical competition increases testosterone among Amazonian forager-horticulturalists: A test of the challenge hypothesis. Proceedings of the Royal Society B: Biological Sciences, 279(1739), 2907–2912. https://doi.org/10.1098/rspb.2012.0100
- Tuljapurkar, S. D., Puleston, C. O., & Gurven, M. D. (2007). Why men matter: Mating patterns drive evolution of human lifespan. PLoS ONE, 2(8), e785. https://doi.org/10.1371/journal.pone.0000785
- Surampudi, P. N., Wang, C., & Swerdloff, R. (2012). Hypogonadism in the aging male diagnosis, potential benefits, and risks of testosterone replacement therapy. International Journal of Endocrinology, 2012, 625434. https://doi.org/10.1155/2012/625434
- Canal de Velasco, L. M., & González Flores, J. E. (2025). Testosterone therapy in men in their 40s: A narrative review of indications, outcomes, and mid-term safety. Cureus, 17(9), e92778. https://doi.org/10.7759/cureus.92778
- Grossmann, M., Jayasena, C. N., & Anawalt, B. D. (2023). Approach to the patient: The evaluation and management of men ≥50 years with low serum testosterone concentration. The Journal of Clinical Endocrinology & Metabolism, 108(9), e871–e884. https://doi.org/10.1210/clinem/dgad180
- Stanworth, R. D., & Jones, T. H. (2008). Testosterone for the aging male: Current evidence and recommended practice. Clinical Interventions in Aging, 3(1), 25–44. https://doi.org/10.2147/cia.s190
- Christensen, L. L., Poulsen, H. E., Andersen, M. S., & Glintborg, D. (2024). Whole-body oxidative stress reduction during testosterone therapy in aging men: A randomized placebo-controlled trial. Andrology, 12(1), 115–122. https://doi.org/10.1111/andr.13458
- Skogastierna, C., Hotzen, M., Rane, A., & Ekström, L. (2014). A supraphysiological dose of testosterone induces nitric oxide production and oxidative stress. European Journal of Preventive Cardiology, 21(8), 1049–1054. https://doi.org/10.1177/2047487313481755
- Bribiescas, R. G. (2006). On the evolution, life history, and proximate mechanisms of human male reproductive senescence. Evolutionary Anthropology: Issues, News, and Reviews, 15(4), 132–141. https://doi.org/10.1002/evan.20086
- Schooling, C. M., & Zhao, J. V. (2021). Investigating the association of testosterone with survival in men and women using a Mendelian randomization study in the UK Biobank. Scientific Reports, 11, 14039. https://doi.org/10.1038/s41598-021-93360-z
- Patel, A. S., Leong, J. Y., Ramos, L., & Ramasamy, R. (2019). Testosterone is a contraceptive and should not be used in men who desire fertility. The World Journal of Men's Health, 37(1), 45–54. https://doi.org/10.5534/wjmh.180036
- Lee, J. A., & Ramasamy, R. (2018). Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men. Translational Andrology and Urology, 7(Suppl 3), S348–S352. https://doi.org/10.21037/tau.2018.04.11
- Smit, D. L., Verdegaal, T., & Bond, P. (2025). Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: A retrospective analysis of real-world data. F&S Reports, 6(2), 120–126. https://doi.org/10.1016/j.xfre.2025.03.001